

How can healthcare organizations develop an effective root cause analysis in healthcare? Read on to learn how your organization can improve outcomes and reduce costs.
What is Root Cause Analysis for Healthcare?
Root cause analysis (RCA) is defined as is a systematic process used to identify and analyze the underlying cause(s) of an issue or problem, with the goal of preventing its recurrence by addressing the root causes rather than only the symptoms.
In a healthcare context, RCA is often applied to investigate adverse events, such as patient safety incidents, to improve care by identifying and correcting the failures in a system or processes, or human errors, that contributed to the event. When done effectively, root cause analysis in healthcare can improve safety, reduce future incidents, and ultimately reduce costs associated with risk.
Creating a safe, fear-free environment for incident reporting is important in order to initiate a thorough Root Cause Analysis. Reporting an incident triggers the initiation of an RCA.
Furthermore, the methodology used to conduct the RCA is important in understanding why an incident happened, and how to prevent it from happening in the future.

Three Questions to Answer
While methodologies may differ, the RCA process is designed to answer three questions:
- What happened?
- Why did it happen?
- What can be done to prevent it in the future?
7 Types of Tools for Root Cause Analysis in Healthcare
1. 5 Whys
This is a simple tool that is appropriately used to get to the root cause of a straight forward problem that does not necessitate the use of advanced statistics. (3) Simply ask the question “Why?” five times, which allows you to discover the root cause of the problem more clearly when you find that the answers to the “Why” questions are interrelated. (2) For example:
-
- Why did the patient break his hip? Answer: Because he fell.
- Why did the patient fall? Answer: Because he lost his balance.
- Why did he lose his balance? Answer: Because he had nothing to hold onto.
- Why was there nothing for him to hold onto? Answer: He was unable to use his walker.
- Why was he unable to use his walker? Answer: The walker was in the closet and not readily accessible for his use.
2. Failure Mode and Effects Analysis
Use this RCA tool to identify which parts in a process are faulty so they can be corrected. It determines the number of times the failure occurs, the actions implemented by the organization to streamline the process in order to prevent the failure from recurring, and if interventions to improve the process were effective. Many organizations use this tool every time a new process is initiated. (2)
3. Fault Tree Analysis
This tool involves the creation of a diagram that looks like a tree where all potential causes of the problem are depicted as branches. (2). Boolean logic, using the terms “And”, “Or”, or “Not”, are applied to each potential cause in order to identify the root cause of the problem. This tool is generally used for complex processes and by those familiar with utilizing Boolean logic. (4) (See Figure 1)
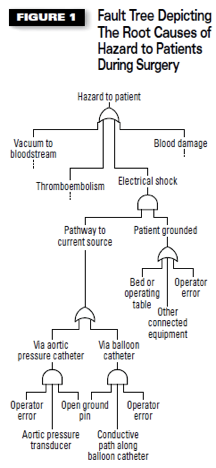
Figure 1
4. Fishbone Diagram
The shape of a fishbone is used to group potential root causes into different sub-categories such as methods, measurements, materials and many others for easier determination of the cause. This tool is relatively easy to use in determining the root cause in complex processes. (2) (See Figure 2)
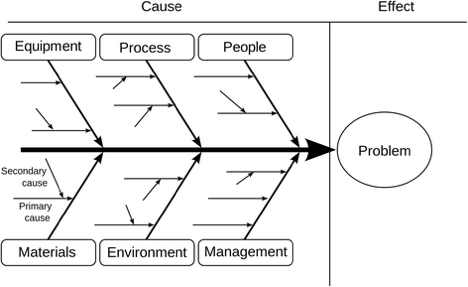
Figure 2
5. Scatter plot or scatter diagram
This a quantitative method of determining if two variables are correlated. This tool is often utilized in combination with the fishbone diagram as a means to test potential root causes. (3)
6. Pareto chart
This is used to group the frequency or cost of different problems to show their relative significance. The bars show frequency or cost in descending order, while the line shows cumulative percentage or total as you move from left to right. Organizations utilize this tool when they want to show the frequency of problems that occur in process or the costs associated with the breakdown of the process. (3)
7. RCA2
Root Cause Analysis Squared was developed by the National Patient Safety Foundation (2015) in an effort to ensure that appropriate and time actions are taken in response to RCA analyses to prevent future harm. The publication is frequently used by health care organizations as a guide on how to conduct efficient and effective RCAs . (5)
The RCA2 process involves specific activities that start with defining which events and close calls are worthy of review and which events are blameworthy. Specific guidelines are prescribed for review team membership and timing of each activity throughout the RCA2 process. There is also embedded into the review process active participation by organizational leadership and a strong emphasis on implementation of steps to reduce the risk of a recurrence of the event.
How do standardized processes and maximize Root Cause Analysis?
Root cause analysis tools in healthcare involves data collection, staff interviews, and literature reviews which culminates in identifying the root cause of a problem and recommendations that will minimize or eliminate the risk of recurrence of the incident.

Many organizations are utilizing technology platforms such as an incident reporting system to ensure they are following a standardized processes when conducting an RCA. Incident reporting software ensure consistency in the RCA methodology used, track the progress of RCAs, alert relevant individuals about progress, manage action items associated with the analysis, and serve as a central repository for information and further learning to prevent the same or similar incidents from occurring again – getting organizations closer to zero harm.
Download our free guide below to learn more about how your organization can implement incident reporting software for effective Root Cause Analysis in healthcare.

Steps Organizations Should Take After Root Cause Analysis
It is important that organizations strategically share the results of their healthcare root cause analysis through training and follow-up action items with the appropriate departments to effectively prevent future errors and reduce the costs associated with the risk of errors.
In addition to sharing the results of the healthcare root cause analysis, organizations are expected to provide the resources and funding to implement the interventions for error prevention that are recommended from the RCA. When personnel see that these action plans are fully implemented, they are more likely to buy-in to incident reporting, participating in the healthcare root cause analysis process, and changing their perception of the patient safety culture of the organization, bringing them closer to zero harm.

Trudi Stafford, PhD, RN, and Clinical Advisor at PHP shares insight on developing processes and tools for effective root cause analysis in healthcare.
Trudi Stafford has 30+ years of health care leadership experience with an emphasis on informatics to positively impact patient safety and health care quality. She is a doctorally prepared nurse executive with prior work experience as the Chief Nursing Office at three of the nation’s largest health systems.
References:
-
Root Cause Analysis. Patient Safety Network. Agency for Healthcare Research and Quality. Retrieved on August 7, 2019 at https://psnet.ahrq.gov/primers/primer/10/root-cause-analysis
-
“What are common Root Cause Analysis (RCA) tools?”. (March 3, 2017). us. Retrieved on August 7, 2019 at https://www.6sigma.us/gsa/
-
Foster, P. (Oct. 30, 2018). 5 Root Cause Analysis Tools for More Effective Problem-Solving. Beacon Quality. Retrieved on August 7, 2019 at https://www.ease.io/5-root-cause-analysis-tools-for-more-effective-problem-solving/
-
“What is Boolean logic?” Lotame. Retrieved on August 10, 2019 at https://www.lotame.com/what-is-boolean-logic/
-
RCA2: Improving Root Cause Analyses and Actions to Prevent Harm. (2015). National Patient Safety Foundation. Retrieved on August 10, 2019
-
What is a Fault Tree Analysis? (March 2002). Quality Progress. Retrieved on August 19, 2019 at http://asq.org/quality-progress/2002/03/problem-solving/what-is-a-fault-tree-analysis.html
-
Gartlehner G, Schultes M, Titscherl V, Morgan, LC, Bobashev, GV, Williams, P, and West SL. (December 2017). User testing of an adaptation of fishbone diagrams to depict results of systematic reviews. BMC Medical Research Methodology. Retrieved on August 19, 2019 at https://link.springer.com/article/10.1186/s12874-017-0452-z
-
Hudgins, JD, Goldberg, V, Fell GL, Puder M, and Eisenberg MA. (November 2017). Reducing Time to Antibiotics in Children With Intestinal Failure, Central Venous Line, and Fever. Pediatrics. Vol 140; Issue 5. Retrieved on August 19, 2019 at https://pediatrics.aappublications.org/content/140/5/e20171201.figures-only
-
Figure 2. Fishbone Diagram Template. Source: Gartlehner G, Schultes M, Titscherl V, Morgan, LC, Bobashev, GV, Williams, P, and West SL. (December 2017). User testing of an adaptation of fishbone diagrams to depict results of systematic reviews. BMC Medical Research Methodology.